
What Is Skin Cancer
Basal cell carcinoma (BCC) is the most common form of skin cancer. BCC tumors typically appear on sun-exposed skin, are slow growing, and rarely metastasize, though neglected tumors can continue to grow and lead to significant local destruction. Chronic, accumulated exposure to sunlight is the most frequent association with the development of BCC.
Squamous cell carcinoma (SCC) is the second most common form of non-melanoma skin cancer and accounts for 20% of cutaneous malignancies. Ultraviolet solar radiation, specifically the cumulative dose of UV radiation received over time, is a major risk factor in the development of cutaneous SCC. Some cases of SCC occur in the absence of a precursor lesion; however, some arise from sun-induced precancerous lesions known as actinic keratoses. SCCs present as papules, plaques or nodules that are skin-colored, pink or red. The surface may be smooth, rough or ulcerated. SCC must be excluded in any non-healing erosion, ulcer or skin lesion that repeatedly bleeds.
Melanoma is a malignant tumor arising from melanocytes and among the most common types of cancer in young adults. Melanomas have 2 growth phases, radial and vertical. During the radial growth phase, malignant cells grow horizontally in the epidermis. Over time, most melanomas progress to the vertical growth phase, in which the malignant cells invade the dermis and develop the ability to metastasize. There are many risk factors, both genetic and environmental that increase the risk of developing melanoma. The main environmental risk factor is excessive exposure of fair-skinned individuals to UV radiation. Individuals with increased numbers of benign melanocytic nevi, large congenital nevi, as well as dysplastic nevi, have increased the risk of developing melanoma. The ABCDs for differentiating early melanomas from benign nevi include the following: A – Asymmetry (melanoma lesion more likely to be asymmetrical), B – Border irregularity (melanoma more likely to have irregular borders), C – Color (melanoma more likely to be very dark black or blue and to have variation in color than would a benign mole, which more often is uniform in color and light tan or brown), D – Diameter (mole < 6 mm in diameter usually benign).
Screening by a dermatologist is extremely important in identifying skin cancers. Early diagnosis and treatment are essential, since skin cancer is highly treatable when diagnosed at an early stage. Patients should be seen by a dermatologist regularly for full-body skin checks and immediately upon noticing suspicious lesions. Treatment options for both SCC and BCC include curettage and electrodessication, excisional surgery, Mohs surgery, topical chemotherapeutic agents, and radiation therapy. Treatment of melanoma is usually accomplished with surgical excision with or without sentinel lymph node biopsy.
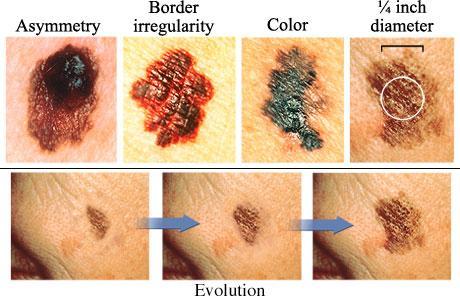
The ABCDEs of melanoma skin cancer are:
- Asymmetry. One half doesn’t match the appearance of the other half.
- Border irregularity. The edges are ragged, notched, or blurred.
- Color. The color (pigmentation) is not uniform. Shades of tan, brown, and black are present. Dashes of red, white, and blue add to a mottled appearance.
- Diameter. The size of the mole is greater than 1/4 inch (6 mm), about the size of a pencil eraser. Any growth of a mole should be evaluated.
- Evolution. There is a change in the size, shape, symptoms (such as itching or tenderness), surface (especially bleeding), or color of a mole.
















